Cholecalciferol and Hysteria
Perpetual Current Events

I originally only wanted to write an update on where research has come with COVID prevention through vitamin D, but the state of the culture seems to be resounding through the science and coverage of the vitamin-hormone. The science community as per the literature on Pubmed seemingly knows core things about the physiology of COVID and its associated outcomes. Likewise, there is significant scientific literature on the physiology of vitamin D, as well as the effects of chronic use.
It turns out the way covid ultimately kills a person, when it does, is typically through thrombosis (microthrombosis specifically), and which substance is intimately involved in inhibiting thrombosis? You could probably guess: Vitamin D. Vitamin D is an inhibitor of thrombin and the coagulation cascade. So why no Fauci, or Biden or other political discussion of the potential?
We do and did have had interventional evidence that vitamin D significantly mitigates influenza prior to COVID-19:
“High-dose vitamin D (1200 IU) is suitable for the prevention of seasonal influenza as evidenced by rapid relief from symptoms, rapid decrease in viral loads and disease recovery”
this was an intervention involving 400 infants in a RCT published in 2018. We also have evidence from multiple correlational outcome studies showing that COVID mortality is inversely associated with blood levels
It is also fairly well known that influenza has a season…generally there is a “flu season” although that was bizarrely up for debate when COVID-19 was terrifying sleep deprived doctors and newscasters. Let's take a look at the cases over time in the US:

A few things undermine the quality of this data, such as the changing definition of what a case is. Initially, the bean counters were accepting all positive COVID tests.. As a data guy I know we do want tests biased towards false positives and we want to account for that, but fixing our counting mistake means we should also restate the original data to be consistent. The decline in Feb, Mar, April 2021 would probably look more like a smooth curve lined up with July 2021 without the re-statement. This winter is just beginning but if Omicron spreads as it has been in other countries we will be set for another peak in late January or early February and then if it behaves like it did in UK and South Africa it will rapidly come back down.
So let's ask our non pharmaceutically biased nephew and niece, when does COVID have the most cases? Would not this fact and the predominant fact of flu being seasonal lead to potentially helpful questions about how seasons impact both virus chemistry and human physiology? Hint - a huge yes it would!!!
The seasonality of COVID or flu generally does not mean that Vitamin D is the solution or the only solution but it’s a huge clue that it is worthwhile to investigate how seasons encourage changes in how diseases spread. Outside of the recent public discourse, we humans know or can readily find out that UV undermines many if not all viruses. We also know that nitric oxide is intimately involved in immune response, and it is released into the vasculature during sun exposure. We even know, if anyone cares to look, that simple body heat is also an important variable for immunity.
So too is vitamin D. There may be other missing factors, but that is a good start for approaching a preventative strategy...if one was actually desired. In my case, I’ve been taking vitamin D, cholecalciferol orally for about 20 years. My current blood levels were just at at 86 ng/dL. The way I get there is by taking 10,000ius also known as ¼ of a milligram per day as well as getting natural sun whenever possible on as much skin as possible. I also “believe” in taking vitamin k2 menaquinone at “absurd” doses of 1mg or more per day along with good amounts of magnesium and zinc, critical cofactors. For COVID specifically I’ve also thrown in quercetin at 4-800 mgs per day.
In my opinion related to self preservation, I “believe” all of these are molecules one can and should take, assuming a desire to live with less disease. That is regardless of a pandemic, so doing so in a pandemic to reduce risk is not for me some new flight to false hope. Apparently most doctors think all non pharmaceuticals might as well be literal snake oil, and many are, but the whole domain is actually out of their scope. Unfortunately, the appropriate experts, naturopaths and biochemists, don’t carry the mystical aura of being medical doctors.
Most of you might not have any idea how medical “science” is made or how much culture and religious thinking are baked into what it is. The medical world is currently obsessed with randomized control trials (RCTs) as the gold standard for evidence based medicine which is how “evidence” is generated as if RCTs have no limitations. Yet, they do have limitations and discernment is still required whether something seems to have support of RCTs or not. To put in more general terms: RCT are one form of empirical evidence, but what most in the medical community have forgotten is that theory and insight need to drive informative empiricism. The way studies are designed, it seems that the existing medical culture is trying to be theory free, or simply theory ignorant. I know most MDs are taught to memorize and the field in general has rejected grand theories. In some ways medicine was or is trying to correct the errors of theory-only-medicine which was also dogmatic and foolish, but the opposite extremis, much like in politics, gets you to the same place. We need the dynamic interplay of both theory and evidence.
Well-powered RCTs are also expensive which bakes in the kinds of things that might ever or never get evidence. That is, substances with the potential for patent protection will have much more funding for the “evidence” of evidence based medicine. In economics this is called a barrier to entry, or a barrier to competition. Big companies love and support rules and culture that keep any nearly free substance in a generally impossible to “provide strong evidence” position. Not logically impossible....Economically Impossible. Ultimately the long term solution requires better institutional design. Probably the government budget should allocate like 4x the amount going into private patentable substances into RCTs for the public good. There are a lot of natural, old, and otherwise un-patentable substances on shelves and on file just un-investigated. Many many more times the amount than novel patentable substances.
The design of RCTs absent appropriate physiological knowledge can offer misleading results. For example, and relevantly, there is a recent and often cited study demonstrating the so-called inefficacy of vitamin-D in relation to COVID-19. They conclude this because a bolus, one shot large dose, didn’t work in the ER to significantly reduce progression or mortality of COVID-19. Perhaps this was a reasonable trial with no mechanistic insight, but it misunderstood the time required to metabolize cholecalciferol and it definitely doesn't really say much about the preventative use of cholecalciferol with enough time to be metabolized. However many doctors, scientists and journalists cite it as though it does. Those supposed to be educated enough are not or they simply want to drive certain results. The appropriate context to test the use of cholecalciferol would be something like 3 or more months of 10,000ius per day with testing to get to levels above 50 ng/dl along with adequate K2 to reduce soft tissue calcification.
Or, as was done in Spain, they should do their homework and use a more appropriate shorter acting metabolite. The Spanish paper, proving even the short term use of D3, was initially retracted and has whispers of intentional suppression, but who would want to suppress a better, lower risk alternative to an mRNA vaccine that needs the non-existence of an alternative for an emergency use authorization?
Anyway, let me summarize key points of evidence in relation to Vitamin D and COVID:
We have interventional RCTs showing that vitamin D reduces the duration and severity of influenza - it was initially not for COVID-19
We have known physiological mechanisms of how vitamin D would reduce the worst effects of COVID
We have various studies showing that mortality decreases in association with blood levels of vitamin D and approaching zero risk at 50ng/dl
We also know that higher levels of vitamin D are associated with lower all cause mortality
We have a previously (but no longer) suppressed RCT study in Spain showing a very significant impact of using an appropriate triage form of vitamin D.
So what do mainstream news and the top North American universities (still) say:
McGill says as a preventative is unsupported on their website by citing a study which is actually rather positive and says among other things: “The efficacy of vitamin D supplements in the prevention of acute respiratory tract infections has best been demonstrated with the chronic intake of low doses, rather than the bolus administration of large doses”
WTF?
Harvard says, “no way!” and they cite: oh no citations…. But they also say, “High doses of vitamin D can cause severe symptoms, such as stomach upsets, kidney injury, and pancreatitis, and may even be life-threatening.” which is sort of true but is only true in extremes…keep in mind two gallons of water can also kill you.
Starting to Smell Something Foul Yet…?
CNN is both pro and anti vitamin D - good job guys
https://www.cnn.com/2020/03/25/health/immunity-diet-food-coronavirus-drayer-wellness/index.html (this one actually cited the BMJ)
The anti article cited a letter of a consensus paper –a consensus paper is CNNs understanding of “science”
MSNBC - also posted on both sides, but mostly describing vitamin D promoting researchers for trying to profit off COVID…right but what do they say about Moderna, Pfizer and the various other “winners” and their profits, but whoa look at all that vitamin D money. (I’m waving my hands)
BBC - Amazing, we might have learned something kind of wonderful:
1) Real journalism still exists - just not in the US.
2) They wrote about the suppressed study in Spain that showed dramatic results, and they note correctly the minimal risk of taking vitamin D. https://www.bbc.com/news/health-56180921
To return to a few people actually trying to aid humanity and public knowledge, the authors of the Spanish study did something logical, and in this world of imbecility, quite clever, they used calcifediol which is one step closer to active vitamin d, calcitriol, because it takes up to 7 days (in normal healthy people) to convert large amounts of cholecalciferol to calcifediol. One wonders in comparison why the US acute study was so poorly thought out and yet its institution has much more brand power. Anyway, what the conclusion from a more intelligent RCT of acute application found was:
“In patients hospitalized with COVID-19, calcifediol treatment significantly reduced ICU admission and mortality.”
Here is a diagram of the vitamin D metabolites:
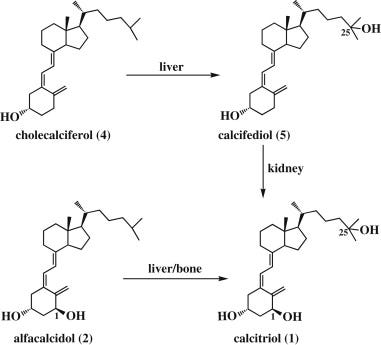
What do you think your chances of getting calcifediol are if admitted in the US, or New Zealand, or probably even in Spain for COVID?
Ivermectin the ole horse dewormer, is to me a sideshow, to be clear, it probably works (the comparative country data seems to make that case), but it should not matter either. Without any prescription or much controversy we, except my mates in New Zealand, have access to very cheap, sufficiently potent vitamin d (along with zinc and quercetin). So what would be a good way to prevent hospital overruns as well as to significantly reduce one’s own risk of mortality?
It’s unfortunate, and none of us want to believe this, but the simple clarity and unknown-ness of the use of oral vitamin D3, or exposed skin in good climates, seems to make the pandemic a catastrophe of cognition (and economic capture of science), and to some extent a self chosen something. I know real lives have been lost, and many people have had non-lethal but horrible outcomes. I don’t mean to imply an outright conspiracy (although the more I read on vitamin D the more plausible political-economic shenanigans seem). At a minimum we have a rather massive pandemic of ignorance, dogmatism and preference for beyond-bad news. The public facing parts of institutions one would expect trust are, in fact, untrustworthy. Are they mired in group think, political tribalism, or a more direct protection of political and financial backers? I can’t really say. I would prefer to invoke Hanlon’s razor: “never attribute to malice what can be attributed to incompetence,” but the level of either ignorance with ideological anti-anything but vaccines or the intentional manipulation of the populace into such a position is very disturbing.
At this moment, I'm trying to shake free of the hypnotism and ponder what it means to have observed and to a small extent participate in such buffoonery. Imagine if the COVID situation was framed as the vitamin D and immune related nutrient deficiency that it (also) is. We might struggle with supply a bit and perhaps have rationing but nothing like the logistics and economic, social, and psychological problems we’ve seen to date, nor the ridiculous power grab of the already have over the terrified have nots.
In a world where we and our institutions do not lust for more fear that would make sense, but that is not the world we live in. The world we live in will never publicly highlight the alternative history, and that collusion involves many of the so-called victims. To victim blame for a second, no-one kept the public from reading the source material about vitamin-d or even purchasing and reasonably ingesting it along with other reasonable cofactors in a COVID mitigation strategy. We were all bamboozled away from thinking and doing our homework as the old institutions auctioned off whatever trust remained for power trips and filthy lucre.
To be clear I sucked it up and got two shots without really thinking about the whole situation until I decided to retool for winter and no longer being covered by the previous shots. I don’t think I have a partisan view. Both teams seem absolutely terrible...I haven’t heard anything from any officials nor any politicians on any side or any medical professional organization outside a few patient focused doctors discussing a coherent non vaccine or combination prevention strategy. Didn’t we want to limit hospital overcrowding...and not kill and unemploy so many people. I get that we don’t really have a public entity to do massive clinical research on non-patentable drugs, chemicals, hormones, etc. but couldn’t we have pulled something together if it was really a crisis. Am I confused here?
Here is a chart from a meta-analysis of 32 studies showing risk of mortality vs vitamin d status:
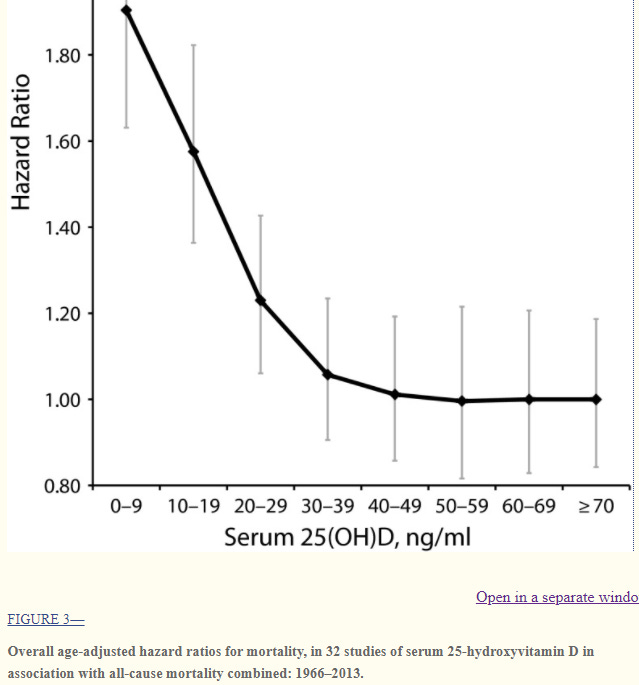
A higher hazard ratio means more likely death, so clearly higher vitamin D to some point 50ish ng/mL means reducing all cause mortality. Do you see the risks of having too high a level? But Harvard posted a fear inducing uncited response to whether one should take Vitamin D to help with COVID.
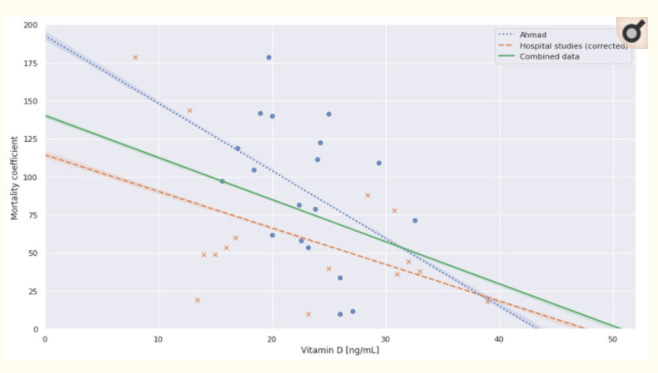
Below is a combination of observational studies looking at mortality specifically from COVID. The model should probably not be linear, but they also don’t have any people with my blood level of Vitamin D in the studies:
Below are some further references, for who, well I don’t know any person that thinks about how crazy I am to put so much stock into one molecule. Take a look it’s all there:
References:
Thrombin generation and fibrin clot structure after vitamin D supplementation
Impact of Serum 25(OH) Vitamin D Level on Mortality in Patients with COVID-19 in Turkey
Vitamin D and COVID-19 severity and related mortality: a prospective study in Italy
The Impact of Vitamin D Level on COVID-19 Infection: Systematic Review and Meta-Analysis
https://en.wikipedia.org/wiki/Calcifediol
Note related to Ivermectin and news anchors: many compounds that are antiparasitic or antifungal, are also antimicrobial, and often may also be antiviral and anti-inflammatory. If you listened to some snooty SOB say something about Ivermectin which is X thus could not be Y they were playing you, and displaying great ignorance. Aspirin antiviral, anti-inflammatory, anti-cancer. Many antibiotics (https://pubmed.ncbi.nlm.nih.gov/12054075/) are anti-inflammatory and thus likely antiviral (Z packs for COVID)... Methylene Blue...anti-parasitic (malaria) and anti-bacterial(sepsis) and a MAOI inhibitor. The list goes on.
Note: The NIH is focused on fundamental research and the FDA is an oversight organization. There are some grants ostensibly through the NIH to do RCTs, but not to run clinical trials for the public domain.
Meta-analysis of All-Cause Mortality According to Serum 25-Hydroxyvitamin D